Description
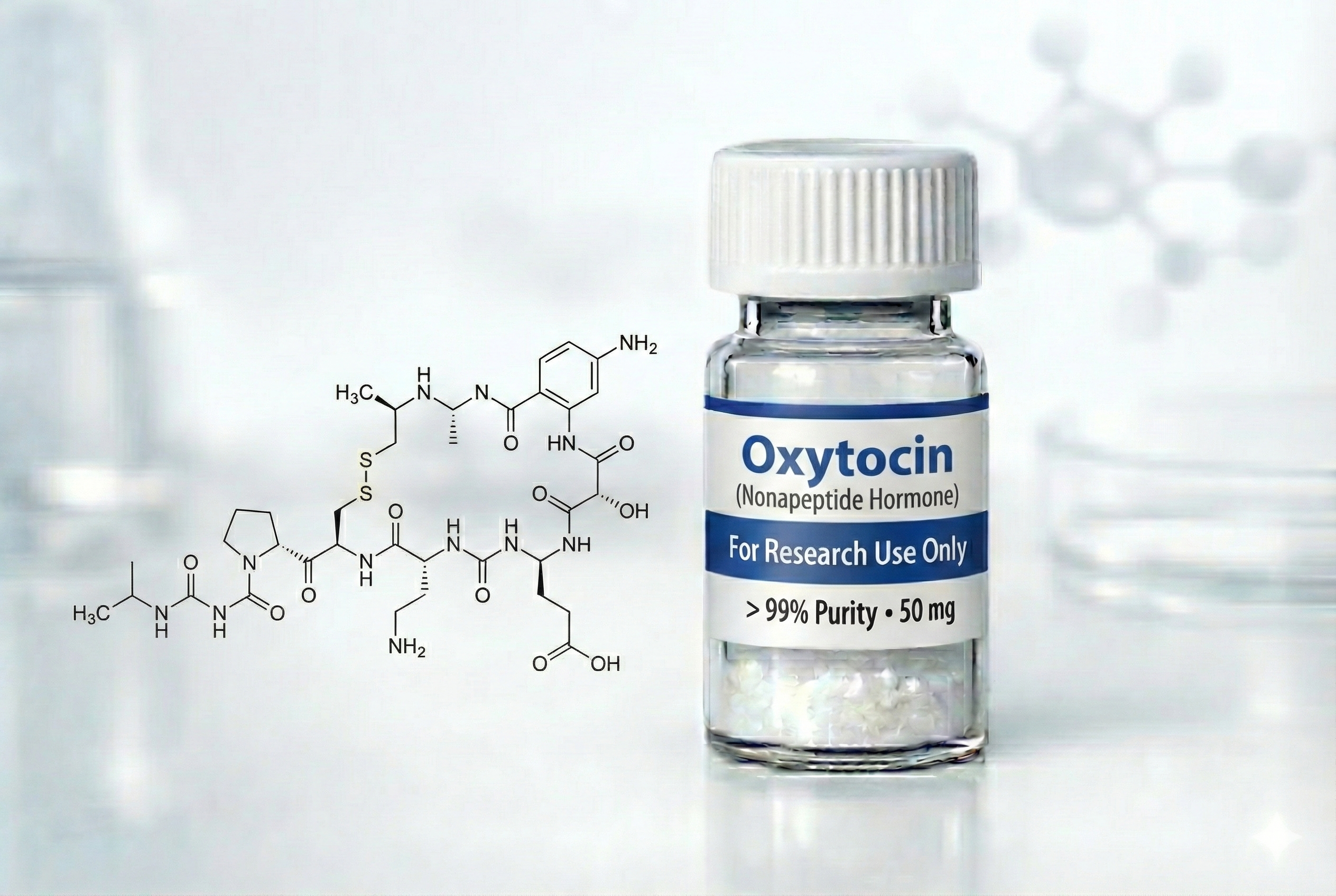
Oxytocin is a naturally occurring oligopeptide hormone consisting of nine amino acids, classifying it as a nonapeptide.¹ The peptide sequence is Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Leu-Gly (with a disulfide bridge between the two cysteine residues), giving it a cyclic structure critical for receptor binding.¹⁰
Endogenous Production and Release:
Oxytocin is synthesized in magnocellular neurons of the paraventricular and supraoptic nuclei of the hypothalamus, then transported via axons to the posterior pituitary gland (pars nervosa) where it is stored and released into the bloodstream.¹ Oxytocin is one of only two hormones stored and released by the posterior pituitary—the other being vasopressin (antidiuretic hormone, ADH).¹
Unlike most hormones that create negative feedback loops, oxytocin exhibits positive feedback: its release stimulates actions that trigger even greater oxytocin release.¹ This positive feedback mechanism is essential for parturition (childbirth) and lactation.¹
Natural Functions:
Parturition (childbirth): The fetal head pressing against the cervix sends nerve impulses that trigger oxytocin release, which intensifies uterine contractions, which in turn triggers more oxytocin release—this escalating cycle continues until delivery.¹
Lactation: Infant suckling stimulates oxytocin release, causing contraction of myoepithelial cells in breast tissue, forcing milk from alveolar ducts into larger sinuses for ejection.¹
Social bonding and attachment: Oxytocin is released during positive social interactions, sexual activity, and physical touch, facilitating pair bonding, parent-infant attachment, and social recognition.²
Stress modulation: Oxytocin dampens HPA axis activity, reducing cortisol release and physiological stress responses.⁶
Receptors and Signaling:
Oxytocin acts through a single G-protein coupled receptor (OXTR) encoded on chromosome 3.² OXTR activation triggers conformational changes leading to G-protein activation (specifically Gq), calcium release from intracellular stores, and downstream effects including smooth muscle contraction, nitric oxide production, vasodilation, and altered neuronal excitability.²
OXTR distribution in the brain is species-specific but generally includes regions involved in social behavior, emotion regulation, and sensory processing—including the nucleus accumbens, amygdala, prefrontal cortex, hypothalamus, and brainstem nuclei.² In prairie voles (a monogamous species studied extensively in oxytocin research), higher OXTR density in the nucleus accumbens is associated with greater partner preference formation.²
Receptor Desensitization:
Both OXTR and vasopressin receptors undergo rapid desensitization via receptor internalization.² In vitro studies suggest >50% receptor internalization can occur within minutes to hours after peptide exposure, potentially limiting sustained effects of exogenous administration.²
Oxytocin vs. Vasopressin:
Oxytocin and vasopressin are structurally similar nonapeptides differing by only two amino acids.² Vasopressin has three receptor subtypes (AVPR1a, AVPR1b/V3, and V2), while oxytocin has one (OXTR).² Despite structural similarity, these neuropeptides have largely distinct effects, though some cross-reactivity can occur at high concentrations.²
Synthetic Forms:
Pitocin (FDA-approved): Synthetic oxytocin identical to endogenous hormone; approved for intravenous/intramuscular administration for labor induction and postpartum hemorrhage control.¹
Syntocinon: Brand name for intranasal oxytocin spray, historically used for milk ejection in the US (now discontinued) and currently used in research studies.⁵
Compounded intranasal oxytocin: Available from compounding pharmacies at 20-30 units/spray for off-label psychiatric/social uses.⁹
Routes of Administration:
Intravenous (FDA-approved): Standard route for obstetric indications; uterine contractions begin within ~1 minute and last ~1 hour.¹⁰
Intramuscular (FDA-approved): Alternative for postpartum hemorrhage prevention; contractions begin within 3-5 minutes and last up to 3 hours.¹⁰
Intranasal (off-label/investigational): Used in psychiatric research studies; purportedly bypasses blood-brain barrier via olfactory and trigeminal pathways to reach CNS structures.⁶ However, whether intranasal oxytocin meaningfully enters the brain remains scientifically disputed.⁸
Pharmacokinetics:
Absorption: IV administration provides complete bioavailability; intranasal administration increases plasma oxytocin from ~21 pg/mL at baseline to ~41 pg/mL at 15 minutes (though CNS penetration remains uncertain).⁹
Distribution: Distributed throughout extracellular fluid; trace amounts may cross placenta.¹⁰
Metabolism: Primarily metabolized by liver and kidneys via the enzyme oxytocinase, which increases during pregnancy.¹⁰
Elimination: Rapidly cleared from plasma; half-life approximately 3-5 minutes for IV administration.¹⁰
Regulatory Status:
United States—FDA Approval:
**APPROVED indications (injectable Pitocin):**¹
- Labor induction in medically indicated circumstances (preeclampsia, maternal diabetes, premature rupture of membranes, post-term pregnancy)
- Labor augmentation (strengthening inadequate contractions)
- Control of postpartum hemorrhage
- Second-trimester abortion (inevitable or incomplete)
**NOT FDA-approved for:**¹
- Elective labor induction (insufficient benefit-risk data)
- Intranasal administration for any indication (previously approved intranasal formulation for lactation was discontinued)
- Psychiatric or social cognitive disorders (autism, BPD, PTSD, social anxiety)
- Sexual dysfunction
- Any non-obstetric indication
Off-Label/Investigational Uses:
Despite lack of FDA approval, intranasal oxytocin is extensively studied and used off-label for:¹
- Autism spectrum disorder (ASD)
- Social anxiety disorder
- Borderline personality disorder (BPD)
- Post-traumatic stress disorder (PTSD)
- Major depressive disorder (MDD)
- Delayed orgasm/sexual arousal disorders
- Couple bonding enhancement
Compounding Pharmacy Availability:
Unlike many investigational peptides, oxytocin is NOT on the FDA’s prohibited Category 2 list, allowing compounding pharmacies to produce intranasal formulations for off-label prescribing.⁹ Typical compounded formulations contain 20-30 units/spray at prices of $70-$80 per bottle.⁹
Institute for Safe Medication Practices (ISMP) Warning:
Despite FDA approval for obstetric use, ISMP classifies oxytocin as one of the 12 most hazardous medications used in hospitals due to approximately 50% of maternity malpractice claims involving alleged oxytocin misuse.¹⁰ Proper monitoring, precise dosing, and trained personnel are essential to prevent complications including uterine rupture, fetal distress, water intoxication, and maternal/fetal death.¹⁰

Reviews
There are no reviews yet.